Monthly Cell Challenge #05 / 2026

What the Smear Revealed
A 68-year-old man was referred to the hematology clinic because of progressive fatigue, reduced exercise tolerance, and a sensation of abdominal fullness that had gradually increased over the previous six months. He also reported intermittent night sweats and an unintentional weight loss of approximately 5 kg during the past year.
The patient denied recent infections or bleeding symptoms. His past medical history included well-controlled hypertension and type 2 diabetes mellitus.
On physical examination, the patient appeared mildly pale. Several enlarged cervical and axillary lymph nodes were palpable. Moderate splenomegaly was also noted.
As part of the clinical evaluation, blood samples were obtained for routine laboratory testing.
CBC results:
| Test | Result | Units |
|---|---|---|
| WBC | 24.8 | x109/L |
| RBC | 3.9 | 1012/L |
| HGB | 112 | g/L |
| MCV | 84 | fL |
| MCH | 28 | pg |
| PLT | 118 | x109/L |
Blood smear analysis classification on CellaVision DC-1
| WBC Differential | % | x109/L |
|---|---|---|
| Neutrophils | 47.3 | 11.7 |
| Lymphocytes | 23.4 | 5.8 |
| Monocytes | 6.3 | 1.6 |
| Eosinophils | 2.4 | 0.6 |
| Basophils | 1.0 | 0.2 |
| Myelocytes | 1.0 | 0.2 |
| Abnormal lymphocytes | 18.5 | 4.6 |
Blood smear findings:
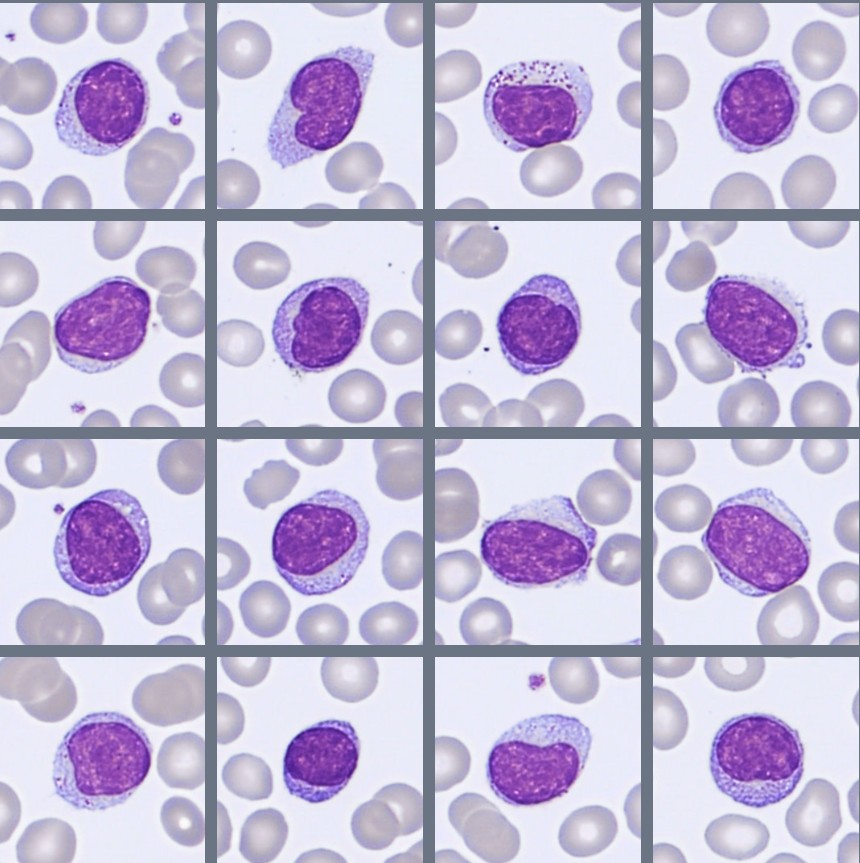
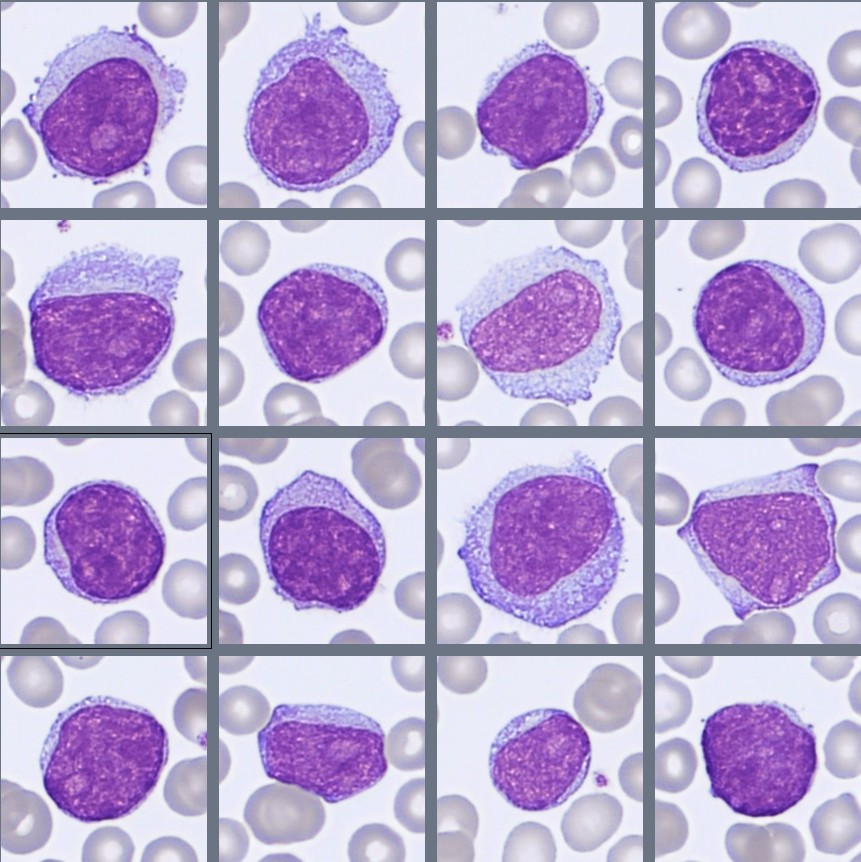
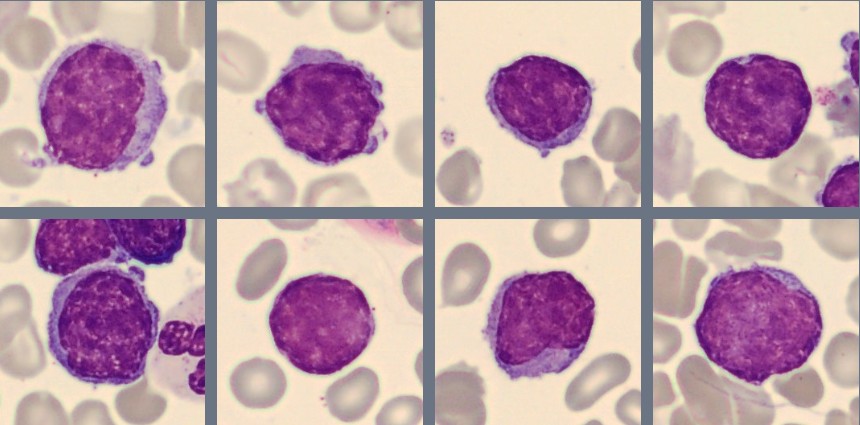
Microscopic examination of the peripheral blood smear demonstrates lymphocytosis with a prominent population of abnormal lymphoid cells.
The abnormal lymphocytes are predominantly medium-sized to large cells with relatively dispersed chromatin and scant to moderate pale basophilic cytoplasm. Some cells display a high nuclear-to-cytoplasmic ratio and visible nucleoli, while a subset of the abnormal lymphocytes demonstrate cytoplasmic projections. The morphology is relatively monotonous, although mild variation in cell size is observed.
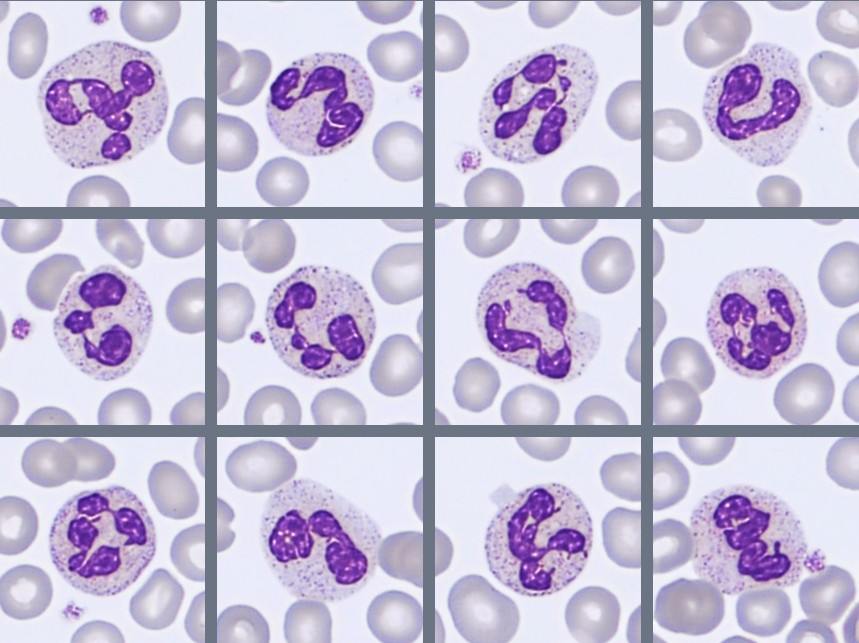
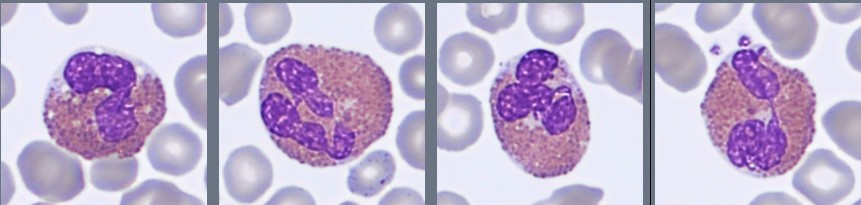
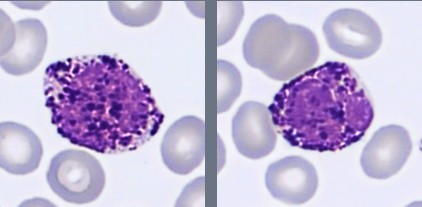
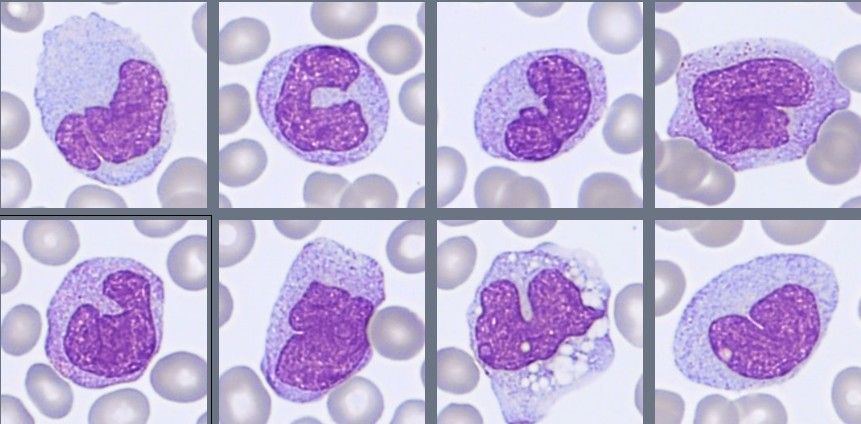
Mature neutrophils show no significant dysplastic features. Occasional eosinophils and basophils are present with normal morphology. Platelets are mildly decreased in number.
The overall blood smear appearance raises suspicion for a mature B-cell lymphoproliferative disorder, prompting further evaluation with bone marrow examination and immunophenotyping.
Bone marrow aspirate findings:
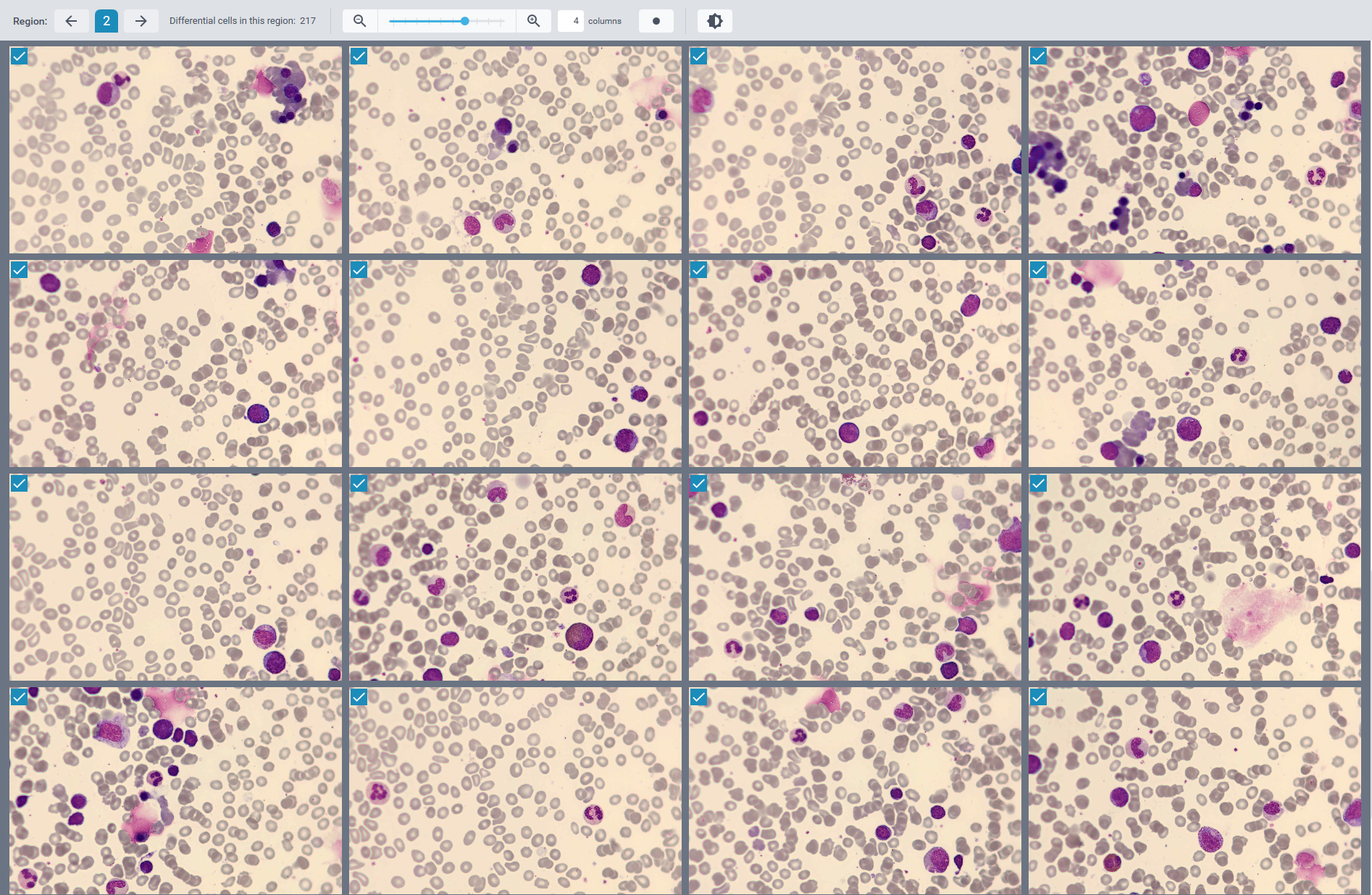
Review of the differential area images of the CellaVision® Bone Marrow Aspirate Application demonstrates slightly increased cellularity and a mild increase in lymphocytes.
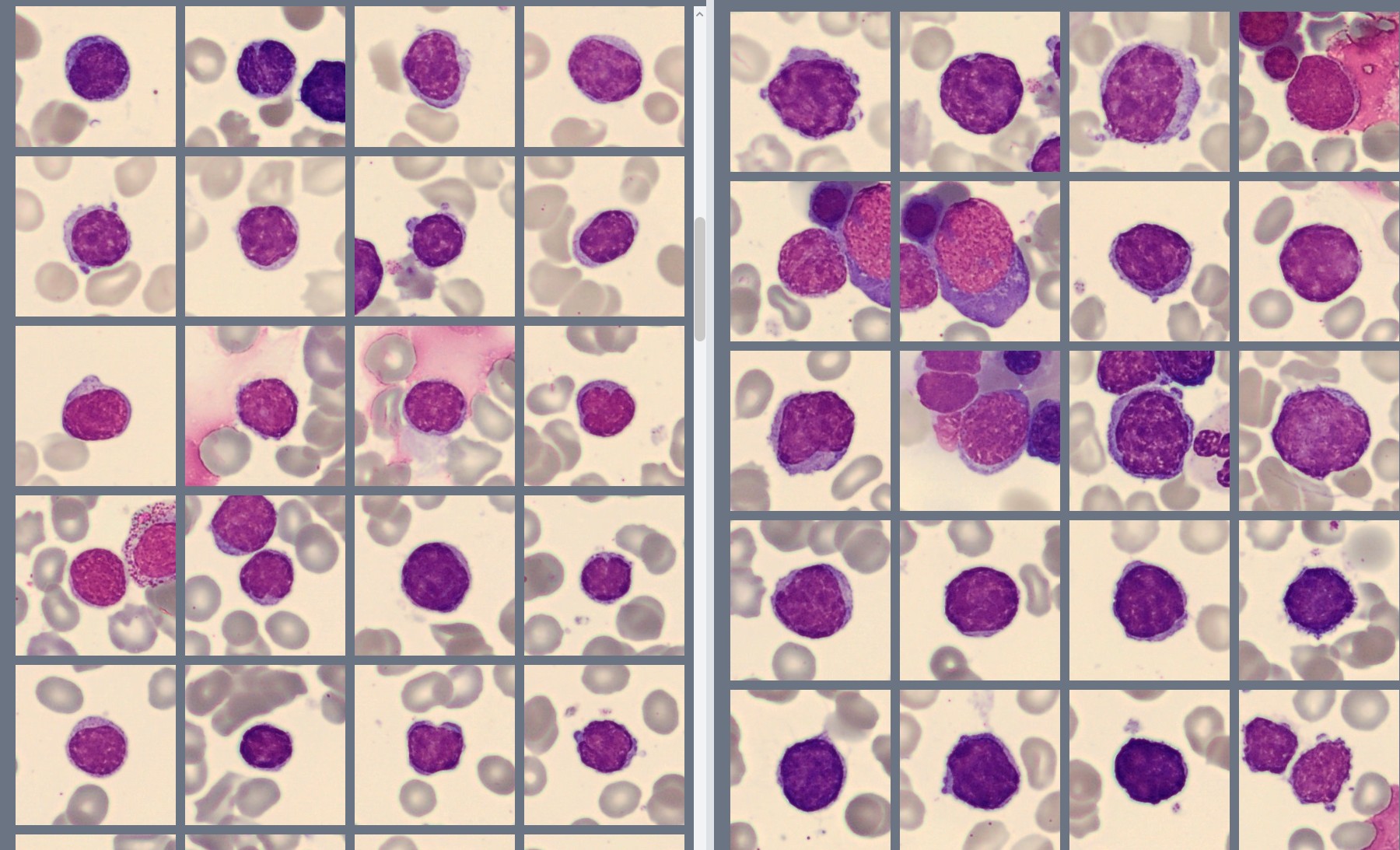
Morphologically, the bone marrow preparations demonstrate the same abnormal lymphocytes as described in the peripheral blood smear.
Erythropoiesis is very active with no noticeable dysplasia. Myelopoiesis is moderately to normally active with sufficient maturation. No significant increase in blast cells is observed.
Bone marrow aspirate differential analysis on CellaVision® BM Aspirate Application:
| Erythroid lineage | ||
| Cell type | Cells | % |
| Proerythroblasts | 1 | 0.2 |
| Basophilic erythroblasts | 4 | 0.8 |
| Polychromatic erythroblasts | 49 | 9.4 |
| Orthochromatic erythroblasts | 98 | 18.8 |
| Total erythroid | 152 | 29.2 |
| Myeloid lineage | ||
| Cell type | Cells | % |
| Blasts | 20 | 3.9 |
| Promyelocytes | 14 | 2.7 |
| Myelocytes | 21 | 4.0 |
| Metamyelocytes | 31 | 6.0 |
| Band neutrophils | 38 | 7.3 |
| Segmented neutrophils | 86 | 16.5 |
| Eosinophils | 15 | 2.9 |
| Basophils | 0 | 0 |
| Monocytes | 4 | 0.8 |
| Mast cells | 0 | 0 |
| Total myeloid | 229 | 44.1 |
| Lymphoid lineage | ||
| Cell type | Cells | % |
| Lymphocytes | 137 | 26.3 |
| Plasma cells | 2 | 0.4 |
| Total lymphoid | 139 | 26.7 |
| Other cells and artifacts | ||
| Cell type | Object | Ratio |
| Macrophages | 0 | 0 |
| Smudge cells | 62 | 11.9 |
| Artifacts | 4 | 0.8 |
Immunophenotyping
Flow cytometric analysis of the bone marrow demonstrates a kappa light chain-restricted monoclonal B-cell population representing approximately 17% of nucleated cells. The abnormal cells express CD19, CD20, CD22, FMC-7, and strong CD5 expression. CD23 expression is weak, while CD10 and CD103 are negative.
Diagnosis:
Mantle Cell Lymphoma (MCL), leukemic phase, WHO 2024.
Discussion:
Mantle cell lymphoma (MCL) is a mature B-cell neoplasm originating from lymphoid cells in the mantle zone of lymphoid follicles [1]. It accounts for approximately 3–10% of all non-Hodgkin lymphomas and most commonly affects older adults, with a median age at diagnosis of around 65–70 years [1,2]. Men are affected more frequently than women [2].
Patients often present with generalized lymphadenopathy, splenomegaly, bone marrow involvement, and peripheral blood lymphocytosis [1,2]. Constitutional symptoms such as fatigue, weight loss, and night sweats are also common. In many cases, the disease is already advanced at the time of diagnosis [1].
The morphology of mantle cell lymphoma can vary considerably. Classical cases are usually composed of small to medium-sized lymphocytes with irregular nuclear contours, condensed chromatin, and scant cytoplasm [2]. In some cases, however, the cells appear larger with a higher nuclear-to-cytoplasmic ratio, more dispersed chromatin, and visible nucleoli, creating a blastoid or pleomorphic appearance [1]. These variants are considered more aggressive and are associated with a higher proliferative rate, more extensive bone marrow and peripheral blood involvement, and a less favorable prognosis [1,4].
Blastoid mantle cell lymphoma can morphologically resemble acute leukemia or other aggressive lymphoid malignancies due to the presence of medium-sized blast-like cells with prominent nucleoli and a high nuclear-to-cytoplasmic ratio [2]. Careful evaluation of morphology, together with immunophenotyping, is therefore essential for accurate classification.
Peripheral blood involvement is common in MCL and may resemble other mature B-cell lymphoproliferative disorders, particularly chronic lymphocytic leukemia (CLL) [2,3].
Morphology alone is not sufficient for diagnosis. Immunophenotyping is essential and typically demonstrates strong expressions of CD20, surface immunoglobulin, FMC-7, and CD5, while CD23 is absent or only weakly expressed [1,2]. A characteristic genetic finding in MCL is the translocation t(11;14)(q13;q32), leading to overexpression of cyclin D1, which is considered a hallmark of the disease [1].
Bone marrow involvement is seen in the majority of patients and may present with diffuse, interstitial, or nodular infiltration patterns [2]. In this case, abnormal lymphoid cells were identified during digital review using the CellaVision® Peripheral Blood Application, prompting further investigation with bone marrow examination and flow cytometry. Review of the bone marrow aspirate using the CellaVision® Bone Marrow Aspirate Application demonstrated the same abnormal lymphoid population seen in the peripheral blood.
Morphologic assessment remains an important first step in the evaluation of hematologic malignancies, but the final diagnosis requires integration of morphology, immunophenotyping, cytogenetics, and molecular findings [1]. Digital morphology systems can support this process by facilitating systematic review and recognition of abnormal cell populations in both peripheral blood and bone marrow specimens.
Treatment depends on patient age, clinical condition, and disease characteristics. Current treatment approaches may include chemoimmunotherapy, BTK inhibitors, anti-CD20 monoclonal antibodies, stem cell transplantation in selected patients, and newer targeted therapies [1,4]. Although treatment options have improved considerably in recent years, mantle cell lymphoma generally remains a relapsing disease [4].
This case illustrates the importance of integrating morphology, immunophenotyping, and clinical findings in the evaluation of lymphoid neoplasms and demonstrates how digital morphology systems support efficient recognition of abnormal lymphoid populations in both peripheral blood and bone marrow specimens.
References:
[1] WHO Classification of Tumours Editorial Board. WHO classification of tumours: Haematolymphoid tumours. 5th ed. Lyon: International Agency for Research on Cancer; 2024.
[2] Bain BJ. Blood cells: a practical guide. 6th ed. Oxford: Wiley-Blackwell; 2020.
[3] Bain BJ, Bates I, Laffan MA. Dacie and Lewis practical haematology. 13th ed. London: Elsevier; 2021.
[4] Campo E, Rule S. Mantle cell lymphoma: evolving management strategies. Blood. 2022;139(24):3323–3335.