CellaVision Global Test 2023:2 - APL
Case Description
39-year-old man was seen in the emergency room with a 2-week history of:
- Progressive weakness
- Fatigue
- Dizziness
- Tiny red spots on the arms and legs
- Widespread bruising
- Bleeding from the gums
Laboratory Findings
| Test | Result | Reference Interval | Unit |
|---|---|---|---|
| WBC | 2.3 | 4.5-11.5 | x109/L |
| HGB | 11.1 | 14-17.5 | g/dL |
| HCT | 33.1 | 40-54 | % |
| MCV | 90.7 | 80-100 | fL |
| RDW | 16.2 | 11.5-15 | % |
| PLT | 7 | 150-450 | x109/L |
| Retic | 3.0 | 0.5-2.5 | % |
| PT | 33 | 11-13.5 | Seconds |
| PTT | 41 | 25-35 | Seconds |
| Fibrinogen | 88 | 200-400 | mg/dL |
| D-Dinner | > 19,000 | < 250 | ng/mL |
Sample of cells classified in the Global Test 2023:2
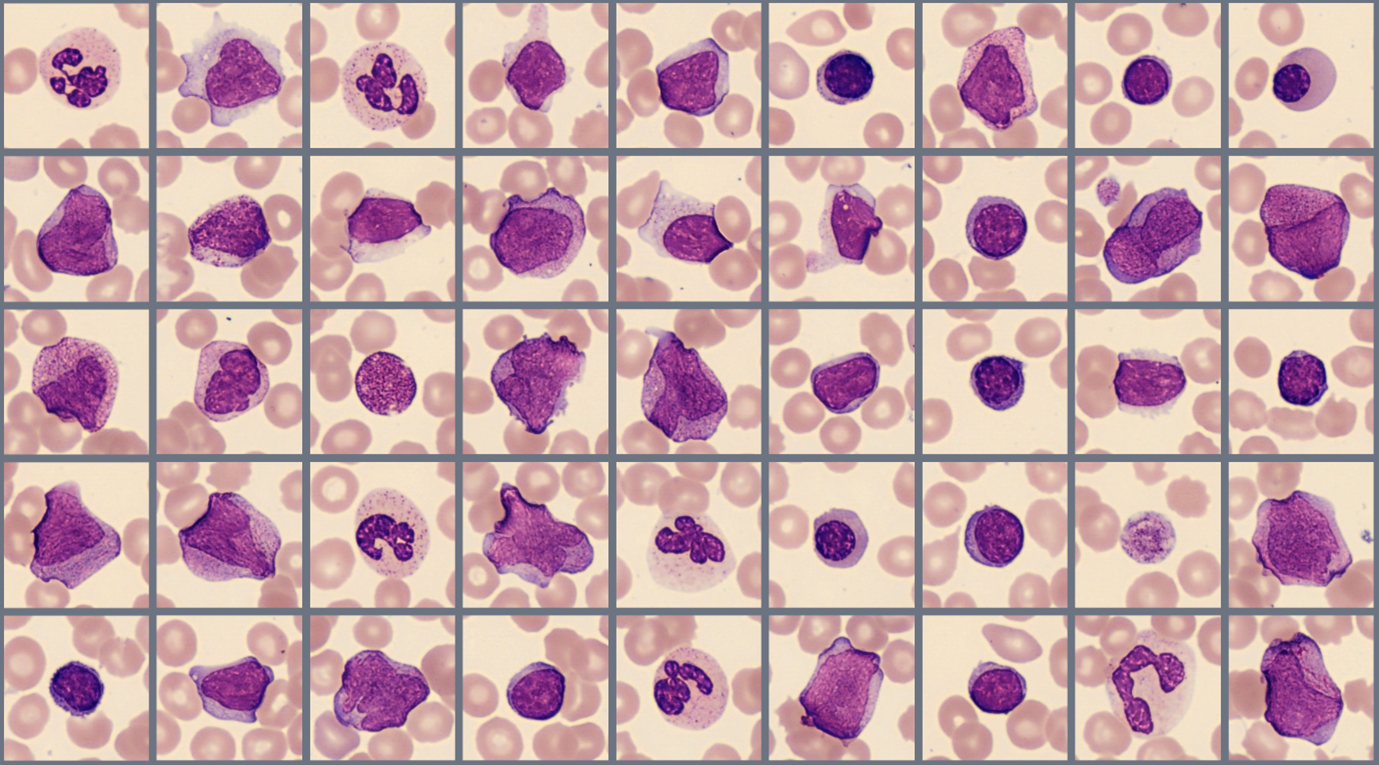
Case Conclusion
The peripheral blood film is suspicious for acute promyelocytic leukemia (APL). Numerous abnormal promyelocytes are present with variable nuclear size and shape; and basophilic cytoplasm with granules that vary in number. Auer rods (often multiple) are visible in roughly 1/3 of the promyelocytes. Several blasts are also noted, however differentiating between blasts and promyelocytes can be challenging. This distinction is not clinically relevant in APL as blasts and promyelocytes are counted together in the WHO classification. Schistocytes are also present, as they are in some APL patients with associated coagulopathy.
Global Test 2023:2 Results Webinar
Questions discussed during the webinar include:
- Why are suspected cases of APL considered medical emergencies?
- Typical clinical and laboratory findings in APL and differences observed in this case.
- Genetic abnormalities that cause APL
- Diagnostic criteria of APL and definition of “blast equivalent.”
- Guidelines for reporting promyelocytes in the WBC differential
- Effect of APL treatment on cell morphology
- APL related coagulopathy